Physicians Mutual Insurance Company®
This affordable dental insurance helps pay for over 400 covered procedures.
View some of the most common procedures and what percentage each plan helps cover — or browse the full list of covered procedures below.
Covered procedures at a glance

| Covered procedure Type | Waiting Period | Economy Plan Coverage | Standard Plan Coverage | Preferred Plan Coverage | Premier Plan Coverage | |
|---|---|---|---|---|---|---|
| pm_checkmark_rounded | Cleanings | None | 100% | 100% | 100% | 100% |
| pm_checkmark_rounded | Routine Exams | None | 100% | 100% | 100% | 100% |
| pm_checkmark_rounded | Dental X-rays | None | 100% | 100% | 100% | 100% |
| pm_checkmark_rounded | Fillings for cavities | None | 25% | 40% | 55% | 70% |
| pm_checkmark_rounded | Minor oral surgery procedures and sedation | None | 25% | 40% | 55% | 70% |
| pm_checkmark_rounded | Simple tooth extractions | None | 25% | 40% | 55% | 70% |
| pm_checkmark_rounded | Root canals | 12 months | 25% | 40% | 55% | 70% |
| pm_checkmark_rounded | Crowns | 12 months | 25% | 40% | 55% | 70% |
| pm_checkmark_rounded | Dentures | 12 months | 25% | 40% | 55% | 70% |
100% coverage for preventive care is only available when you see an
in-network dentist.
The 25%/40%/55% are averages of the maximum allowable charge. 70% is what
we’ll pay of the maximum allowable charge.
See list of all covered procedures
- Each plan pays 100% for preventive (type I) services when you see an in-network provider.
- The Premier Plan (Schedule 4) pays 70% of the maximum allowable charge for basic (type II) and major (type III) services.
- The other three plans – Preferred (Schedule 3), Standard (Schedule 2) and Economy (Schedule 1) – pay a set dollar amount, for basic and major services. With these three plans, the amounts shown for basic and major services are the same regardless of provider participation.
- For Participating Providers, the amount paid will not exceed the Maximum Allowable Charge. For Non-Participating Providers, the amount paid will not exceed the amount of the actual charge for the procedure.
| Type I - Preventive 100% covered preventive care only at network providers. | |
|---|---|
Code D0120 Description Periodic oral evaluation – established patient. ECO STA PRE PRM | 100% |
Code D0145 Description Oral evaluation for a patient under three years of age and counseling with primary caregiver. ECO STA PRE PRM | 100% |
Code D0150 Description Comprehensive oral evaluation – new or established patient. ECO STA PRE PRM | 100% |
Code D0180 Description Comprehensive periodontal evaluation – new or established patient. ECO STA PRE PRM | 100% |
| Two evaluations will be allowed in a Policy Year. A D0120, D0145, D0150 or D0180 counts toward this maximum allowance. D0150 and D0180 will be limited to once per provider. | |
Code D0210 Description Intraoral – complete series of radiographic images. ECO STA PRE PRM | 100% |
Code D0330 Description Panoramic radiographic image. ECO STA PRE PRM | 100% |
| D0210 or D0330: One of these procedures will be allowed in a 5-year period.* | |
| Type II - Basic |
|---|
Code D0140 Description Limited oral evaluation - problem focused. ECO STA PRE PRM** $11 $18 $25 70% |
Code D0170 Description Re-evaluation - limited, problem focused (established patient; not post-operative visit). ECO STA PRE PRM** $11 $18 $25 70% |
| D0140 and D0170: Coverage is limited to accidental injury only. If not due to an accident, will be considered as a D0120 and count toward this maximum allowance. |
Code D0472 Description Accession of tissue, gross examination, preparation and transmission of written report. ECO STA PRE PRM** $18 $28 $38 70% |
| Type III - Major |
|---|
Code D3220 Description Therapeutic pulpotomy (excluding final restoration) – removal of pulp coronal to the dentinocemental junction and application of medicament. ECO STA PRE PRM** $23 $36 $49 70% |
| Limited to the treatment of primary teeth: |
Code D3221 Description Pulpal debridement, primary and permanent teeth. ECO STA PRE PRM** $23 $36 $49 70% |
Code D3222 Description Partial pulpotomy for apexogenesis – permanent tooth with incomplete root development. ECO STA PRE PRM** $38 $61 $84 70% |
Code D3230 Description Pulpal therapy (resorbable filling) – anterior, primary tooth (excluding final restoration). ECO STA PRE PRM** $38 $61 $84 70% |
Code D3240 Description Pulpal therapy (resorbable filling) – posterior, primary tooth (excluding final restoration). ECO STA PRE PRM** $38 $61 $84 70% |
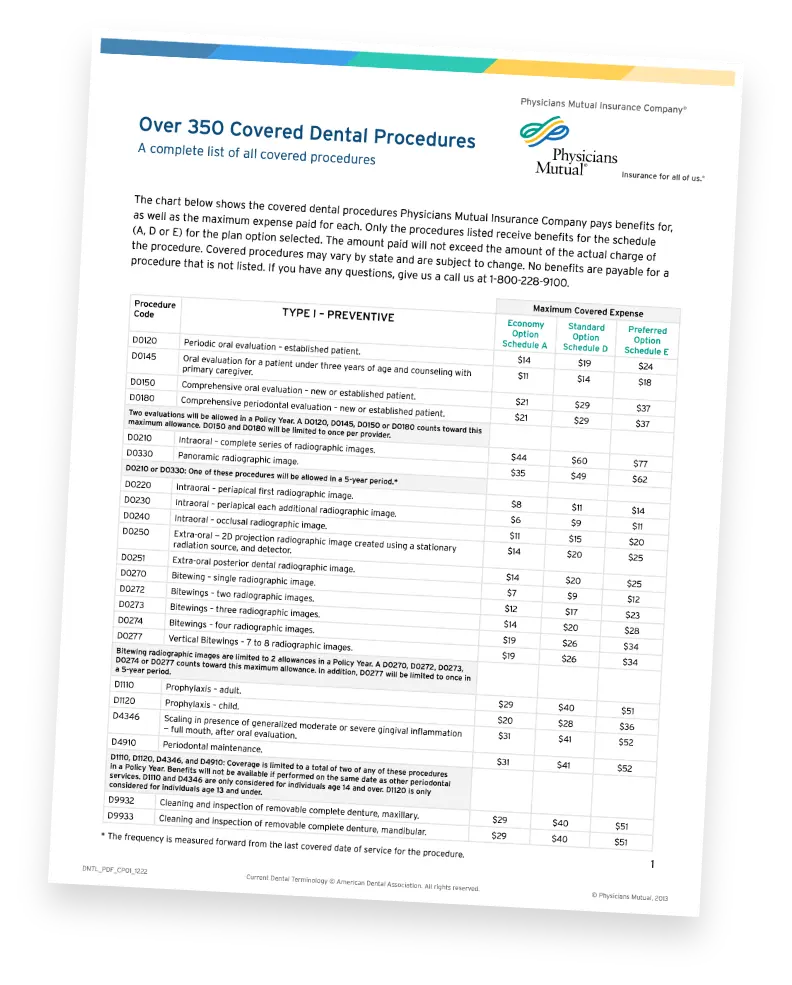
Type I - Preventive 100% covered preventive care only at network providers. | Maximum Covered Expense | ||||
|---|---|---|---|---|---|
| Code | Economy Schedule 1 | Standard Schedule 2 | Preferred Schedule 3 | Premier Schedule 4 | |
| D0120 | Periodic oral evaluation – established patient. | 100% Covered | |||
| D0145 | Oral evaluation for a patient under three years of age and counseling with primary caregiver. | 100% Covered | |||
| D0150 | Comprehensive oral evaluation – new or established patient. | 100% Covered | |||
| D0180 | Comprehensive periodontal evaluation – new or established patient. | 100% Covered | |||
| Two evaluations will be allowed in a Policy Year. A D0120, D0145, D0150 or D0180 counts toward this maximum allowance. D0150 and D0180 will be limited to once per provider. | |||||
| D0210 | Intraoral – complete series of radiographic images. | 100% Covered | |||
| D0330 | Panoramic radiographic image. | 100% Covered | |||
| D0210 or D0330: One of these procedures will be allowed in a 5-year period.* | |||||
Type II - Basic | Maximum Covered Expense | ||||
|---|---|---|---|---|---|
| Code | Economy Schedule 1 | Standard Schedule 2 | Preferred Schedule 3 | Premier Schedule 4** | |
| D0140 | Limited oral evaluation - problem focused. | $11 | $18 | $25 | 70% |
| D0170 | Re-evaluation - limited, problem focused (established patient; not post-operative visit). | $11 | $18 | $25 | 70% |
| D0140 and D0170: Coverage is limited to accidental injury only. If not due to an accident, will be considered as a D0120 and count toward this maximum allowance. | |||||
| D0472 | Accession of tissue, gross examination, preparation and transmission of written report. | $18 | $28 | $38 | 70% |
Type III - Major | Maximum Covered Expense | |||||
|---|---|---|---|---|---|---|
| Code | Economy Schedule 1 | Standard Schedule 2 | Preferred Schedule 3 | Premier Schedule 4** | ||
| D3220 | Therapeutic pulpotomy (excluding final restoration) – removal of pulp coronal to the dentinocemental junction and application of medicament. | $23 | $36 | $49 | 70% | |
| Limited to the treatment of primary teeth: | ||||||
| D3221 | Pulpal debridement, primary and permanent teeth. | $23 | $36 | $49 | 70% | |
| D3222 | Partial pulpotomy for apexogenesis – permanent tooth with incomplete root development. | $38 | $61 | $84 | 70% | |
| D3230 | Pulpal therapy (resorbable filling) – anterior, primary tooth (excluding final restoration). | $38 | $61 | $84 | 70% | |
| D3240 | Pulpal therapy (resorbable filling) – posterior, primary tooth (excluding final restoration). | $38 | $61 | $84 | 70% | |
* The frequency is measured forward from the last covered date of service for the procedure.
** 70% of the maximum allowable charge